Health Care in the U.S.
Irene Ngun
Biology Senior Seminar
Outline
I. Introduction
II. The System
A. History: How the market-driven system began and how health care policies are made
III. System inefficiencies and inequities
V. Conclusion
Thesis: Compared to a market-driven health care system, universal health care can do a better job of making adequate service available to everyone. However, universal health care is not a plausible solution in America’s political environment.
U.S. Health Care: Where we stand
The U.S. health care system is an ongoing topic of debate. Much of the debate concerns the access, efficiency, quality, and cost of health care. In 2000, the World Health Organization ranked the U.S. 37 out of 191 countries assessed for their health care performance, landing just above Slovenia. Considering the United States’ ever-soaring GDP and non-stop technology expansion, this is very poor performance. However, in a National Heal Interview Survey carried out by the Center for Disease Control and Prevention (2007), researchers say in 2006, the percentage of persons who were satisfied with their health care program was 65.9%. Even though this number may seem to represent the majority, it is important to note the remaining 34.1% that find themselves underinsured. Today, there are sixty two million of underinsured and uninsured individuals (Lewin & Baxter, 2007, p.1492). With this many individuals unable to afford adequate care, advocates of universal health care are starting to vocalize their opinions. These opinions are more vocal today than they were in previous years partly because of
the upcoming presidential election.
Michelle Andrews of U.S. News (2007) reported that health care reform ranks second to the war in Iraq among issues Americans would like to hear the presidential candidates talk about, proving that people are becoming increasingly concerned about the state of their health care program. While these opinions and proposals of health care reform are funneled into the offices of members of congress, politicians—particularly those involved in the 2008 presidential campaign—are utilizing facts and statistics to sever their political agenda. To compete, each candidate proposes some kind of health care plan that would alleviate the enormous cost that citizens have to pay. However, universal health care is almost unheard of in their big talks about health care reform due to its “economic implications”.
In the age of information, the public mind is very easy to shape. Luring, false promises about a new health care plan is easy bait for people who know very little on health care policy. Before concluding what reform plan is most adequate to our current system, many aspects of health care should be considered: its history, current state, economic efficiency, and most importantly, the cost of universal health care if it were to be implemented.
II. The System
Policy making in the U.S., as described by B. Guy Peters in his book American Public Policy (2007), is dominated by incrementalism, a type of policy making where drastic changes are avoided to minimize risks. Incrementalism is an ancient concept that can be dated back to the days of our property obsessed founding fathers. As much as one would like to believe that policy making is pluralistic in its approach, there is too much evidence that says otherwise. This is very evident in the way health care polices are made since the establishment of governmental, quasi-governmental, and private agencies in the U.S.
A. History
The health care system in the U.S. began to take shape during the presidency of John Adams in 1798, when he established the first Marine Hospital. Soon afterwards public and private agencies started to sprout, one of them being the American Medical Association (AMA). AMA was founded by a young New Yorker, Dr. Nathan Davis, who was only in his thirties when the association was established. AMA’s mission as stated on its website is “To promote the art and science of medicine and the betterment of public health.”. Early in the nineteenth century, soon after its establishment, the AMA supported federal role in public health care activities. However, the increased role of the central government posed as a threat to the economic interests of physicians. Since then, the AMA has been the most viscous opponent of all health care reform proposals that include some kind of governmental activity.
Unlike many European countries such as Sweden, Denmark, and Switzerland in the 1900s, the United States had a very limited role when it came to public health. This was reflective of the ideology the nation had been founded on: classical liberalism, a doctrine that came about from academic scholars such as Charles Montesquieu, John Locke, and Adam Smith. Classical liberalism holds the idea that there should be constitutional limitations on governmental role in public activities. Hence, the government was very decentralized and had unnoticeable role in promoting social welfare.
Health insurance did not become a political issue until the United States’ involvement in World War I. The situation then resembles much of what is happening today. Progressives were pushing for a health care reform that would give compulsory health insurance, however, on the other side, AMA and its band of physicians, followed by pharmaceutical and insurance companies were pushing just as hard to prevent any laws to pass. In 1921, the Sheppard-Towner Act was developed and endorsed by children’s advocates. This act called for federal grants for local child health clinics. Seven years after its legislation, however, the Sheppard-Towner Act was terminated by congress after much kicking and screaming from AMA and the Supreme Court. In 1922, the AMA House of Delegates called the act “an imported socialistic scheme” (Stanley, 1969, p.781) while the Supreme Court deemed Sheppard-Towner as “unconstitutional”a.
With many obstacles, the federal government did succeed to expand its role—incrementally, of course, in public health care during the 1930s, notably because of the Great Depression, which caused problems that were far too large to be handled by the state. A significant event occurred in the 30s when President Franklin D. Roosevelt endorsed the Social Security Act, which provided unemployment compensations, old-age pensions, and other benefits. Originally, the act had also included a form of national health insurance, however, in fear that AMA’s relentless opposition might jeopardize the passing of the act, any mentions of health care was omitted.
It is important to note, that health care reform has been, if not the central issue, one of the top issues addressed by almost all presidential candidates, especially after the Great Depression. Before Franklin D. Roosevelt, it was President Coolidge who appointed committees to investigate health care inefficiencies, much of which we still feel today. The committees found that many Americans were unable to afford medical care and suggested a health care reform in which medical care would by paid through taxation. AMA, not surprisingly, responded by attacking the plan, claiming it an act of “socialism and communism—inciting to revolution” (Koojiman, 1999, p.37).
The ideas for health care reform that were dropped during Franklin D. Roosevelt’s presidency became the basis of the Murray-Wagner-Dingell bill of 1945 that was endorsed by President Truman. This bill called for congress to enact national health insurance funded by payroll deductions. Again, AMA’s intervention was enough to prevent the bill from being passed in congress. As stated by Peter Corning, “On the heels of President Truman's election victory, an 'Armageddon' psychology set in within the AMA. In December 1948, the AMA's House of Delegates met, in an atmosphere of crisis and voted a special assessment of $25 per member to resist 'the enslavement of the medical profession.' A prominent public relations firm was hired and a $4.5 million fund was deployed to wage a 'national education campaign' against the Wagner-Murray-Dingell bill. The campaign included publicity through the mass media, nationwide distribution of pamphlets, a vast speechmaking effort, and a drive to win and publicize specific pledges of support for the AMA's position from the press and other private organizations.”(1969). Although Truman failed to have the bill passed, he did manage to form plans that became the basis of what we know now as Medicare (Stoiber, 2002).
In 1963, President Kennedy proposed thirty-nine legislative recommendations for senior citizen aid. Through this proposal he addressed the need of Medicare to meet the medical needs of those who are eligible for Social Security, mainly the elderly. Unfortunately, President Kennedy was assassinated before congress had the chance to look at the proposals. President Lyndon Johnson also made health care a priority and took advantage of the Medicare plan left by Kennedy. In 1965, Medicare and Medicaid was adopted to the Social Security Act of 1935 as amendments after a long compromise, mainly among three groups: the Johnson administration, Congress’ Republican party, and AMA (Patel & Rushefsky, 2006).
Once Medicare and Medicaid were enacted by the states, access to health care increased significantly. However, increase in access lead to a dramatic increase in cost. By the 1970s, the nation’s expenditure on health care more than tripled. Today the United States, the world’s largest economy, spends 15% of its $13 trillion GDP on health care alone. It is clear that not much has changed from the establishment of the first Marine Hospital in 1798. Two hundred years has passed and yet the U.S. still faces the same problems of access and inefficiency. The only notable change in health care today is its painfully enormous cost.
1. Government
Although it seems that the government has little to no role in public health, it is important to note that about 44% of health care in the U.S. is funded by the government. In addition to that, a good portion of a physician’s wage—including those that endorse an exclusively private health care system—are provided by the government (Peters, 2007). Listed below are examples of governmental roles in public health care.
Medicare and Medicaid
Established in 1965, Medicare and Medicaid, became permanent fixtures of the Social Security Act of 1935, as described in the previous section. Medicare is essentially a program that provides medical insurance for elderly and disabled people who are eligible for Social Security. Medicaid, on the other hand, is a program that provides federal matching funds to state and local governments for medical care of welfare recipients and those who qualify for Medicaid assistance according to laws of their particular state. Often times, a state can choose not to use Medicaid at all. In many cases, however, the federal government does not provide enough funding for the state. Medicaid budget differs from one state to another and often times, and this is mainly caused by the increased cost of health care and increased need of access, the state must raise taxes to accommodate for the shortcomings of federal subsidies. In the state of Indiana, for example, the tax for a pack of cigarettes has been raised from what used to be 44 cents to 99.5 cents in order to pay for Medicaid. The table below describes four components of Medicare, which the enrollee may choose from.
Table 1. Four components of the Medicare program (medicare.gov, 2007)
Components |
Time of Enactment |
Coverage |
Part A |
1965, with the legislation of Medicare and Medicaid |
Hospital insurance (mainly for hospital stays) |
Part B |
1965, with the legislation of Medicare and Medicaid |
Medical insurance (physician, nurses, and other services not covered in part A) |
Part C |
1997, with the passage of the Balanced Budget Act |
An option to receive part A&B from a private health insurance company |
Part D |
2006, with the passage ofMedicare Prescription Drug, Improvement, and Modernization Act |
A plan that cover drug costs with co-payment. |
Health Maintenance Organizations
Health Maintenance Organizations (HMO) entered the picture during Nixon’s administration. The Health Maintenance Organization Act was passed in 1973. HMOs are a system in which enrollees pay a fixed fee in advance in order to receive health services. The Nixon administration believed that HMOs would shift health care from more costly inpatient services to a less costly outpatient service system. Although the HMO Act of 1973 clearly states that in order to be regarded an HMO, an organization must be structured to be non-profit, an increasing number of managed care organizations have become for-profit. A report released by the Kaiser Family Foundation revealed that the number of HMO enrollees that were a part of a non profit HMO decreased from 88 percent in 1988 to only 37 percent in 1997. Opinions of HMOs are divided. On one hand, the opponents of for-profit HMOs say that the system is inefficient and its quality questionable. There is also great concern caused by the fact that for-profit HMOs tend to deny health services to their enrolled patients due to very vague reasons. However, on the other hand, HMOs have had some success in “restraining costs, avoiding unneeded surgeries, promoting prevention” (Easterbrook, 1997).
SCHIP
SCHIP, the State Children’s Health Insurance Program was in some ways an expansion of a previous legislation, the Health Insurance Portability Act and Accounting Act of 1996 which basically placed limits on insurance companies’ ability to deny coverage. SCHIP was endorsed by Senator Hillary Rodham Clinton and Senator Edward Kennedy in 1997. This program is structurally similar to Medicaid with the exception that it is aimed for uninsured children. As of 2006, SCHIP covers about 6.9 million children. Earlier this year, SCHIP expansion has been hot topic of debate in congress (CDS, 2006). The Children’s Health Program Reauthorization Act of 2007 was proposed this past February by both houses of congress. This bill called for the expansion of SCHIP, which required an extra budget of $35 billion over the span of 5 years (CBO, 2007). The bill was vetoed by the President in October because of its threat of leading to socialized medicine.
2. Private Sector
The United States has a mostly private health care system. Employees and their dependants usually receive their health insurance plans from employers who have some kind of agreement with an insurance company. In fact, a report from the Commonwealth Fund Organization revealed that about 55 percent of the 296.8 million individuals in the U.S. receive health insurance from their employers and only 4 percent can afford to purchase health insurance from a private company, the rest are either completely covered by the government (Medicare or Medicaid) or uninsured (2007). Almost all the health services in the United States are administered in private hospitals and by private doctors.
III. System Inefficiencies and Inequities
As Kant Patel and Mark Rushefsky put it, just because policymaking is gradual, that does not mean that it is uncontroversial or unproductive. The U.S. spends 15 percent of its national income on health care, making the U.S. ranked first out of 190 countries in national expenditure. Sadly, being ranked the first does not mean the U.S. has an extraordinary health care system, as we are ranked 37th in health care performance. Listed below are some of the inefficiencies and inequities that have come about from the system the government has chosen.
1. Increased Use of Emergency Care
A recent survey done by the Center for Disease Control and Prevention (CDC) observed the usage of ambulatory medical care across physician offices, hospital emergency rooms, and outpatient departments. The survey revealed that uninsured individuals are less likely to seek for health care, whether that is regular check-up or preventive care. Due to the likelihood to delay search for medical assistance, the individuals’ medical crises usually accumulates, resulting in emergency hospitalization which ends up being more expensive than the cost for preventive care (2007).
2. Shared Costs of the Uninsured
The cost of treating the uninsured often times fall into the hands of taxpayers and those who are insured through higher premium rates. To many, this is unfair. According to a comprehensive study done by the American College of Physicians, in 2001, the total dollar value of care received by the uninsured was half of that received on average by privately insured individuals, despite the fact that about $35 billion went into “uncompensated care” in 2001 alone. This cost is borne by the health care system, that is, hospitals, community clinics or health centers, and physicians (2004).
3. Administrative Cost
According to study done by Harvard Medical School and the Canadian Institute for Health, about 31 percent of U.S. care dollars or in other words, more than $1000 per person per year went into administrative costs, a far higher amount of money that is spent by Canada with its single-payer system (2003). Administrative costs include the cost of adjusting claims, medical bills, hospital supplies and facilities, etc.
B. Inequities
Injustice arises from anything that a group of people deems a luxury instead of a right. Health care in the U.S. is a good example. With the rise of for-profit HMOs and increase cost of health care, inequities arise. Listed below are two inequities that are the most apparent in the U.S. health care system.
1. Medical Underwriting
Medical underwriting is a term health insurance companies use to refer to medical background check. This background check is conducted in order to determine whether or not the candidate for insurance is qualified for coverage. In many cases, an insurance company may deny coverage because of a “pre-existing condition”. Or in other cases, due to a certain condition, a candidate must pay higher premiums or purchase an extra plan.
2. Coverage Gaps
The next notable inequity is the problem of coverage gaps. In this section, it becomes clear how poorly designed the U.S. health care system is. The majority of the health care system is dominated by for-profit HMOs such as Kaiser Permanente and Humana, and by other health insurance companies that are free to set their own premium rates and limitations. The rest, the 44 percent of the system, is run by the government through Medicare, Medicaid, and SCHIP. There are those, unfortunately, that are unable to purchase private insurance but make too much money to qualify for Medicaid. A study done by the Commonwealth Fund earlier this year found that 37 percent of adults in the U.S. have delayed seeking for care due to costs (2007).
IV. Alternative Systems
According to Patel and Rushefsky there are three major models of health care. The first is mostly private, like what the U.S. has. The second is mostly public and health care is paid through taxation. This is the type of system that is used by Great Britain, Sweden and Italy. The third type is a hybrid system, in which health care is mostly publicly funded by delivered by private hospitals and physicians. This model is used by countries such as Japan, Canada, and France.
Reading through other articles and books, one might find it difficult to understand which model is used by which country as phrases such as universal health care, national health care, single payer system, and socialized medicine are tossed around interchangeably. The diagram below, provided by Wikipedia, is a concise description of different models of health care systems.
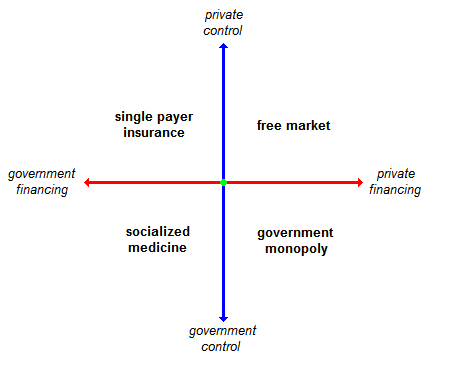
Figure 1. Health care systems. (1st quadrant is the single payer insurance and is read clockwise)
As seen in figure 1, the U.S. health care system falls between the 2nd and 3rd quadrant. The single payer system, although popular among the citizens, are not exactly free of flaw. In fact, all of these systems are not flawless. The British National Health Service (NHS), for example, has been widely criticized for its poor quality of service (BBC, 2005). B. Guy Peters also mentions that universal access to health care may not necessarily solve the poor quality of health in the U.S. as it is observed in the U.K. where gaps of health quality between the poor and the middle class are still very apparent.
Arguments on Universal Health Care
The health care system consists of many actors and players: the powerful AMA, the insurance companies, pharmaceutical and drug industry, politicians and etc. Although universal health care may look like the most logical answer to the access and efficiency problems the U.S. faces, is important to remember the incrementalism that dominates the political system. Listed below are some arguments against and for universal health care.
Arguments against universal health care
- That health care is a right for every human being is a socialized medicine myth (Goodman, 2005).
- As in the case of the NHS of Great Britain and many other countries, the waiting time for medical care will increase as access increases, leading to unnecessary deaths.
- As mentioned by Peters, there will still be health care disparities even with universal access.
- The system may lead to the loss of private practices and reduced income for physicians and health care workers alike. Or as the AMA puts it, “enslavement of the profession”.
- The system will lead to more paperwork due to overregulation by the government which will lead to a decline in quality and inefficiency.
Arguments in favor for universal health care
- Health care should be provided regardless of one’s income because it is a basic right, as cited by the United Nations in Universal Declaration of Human Rights of 1948.
- A comprehensive study on U.S. health care expenditures shows that with the universal health care system, the government will be able to save $286 billion on paperwork alone.
- With less money put into administrative cost, doctors will be able to focus more on their patients. This would lead to an upward trend in quality and efficiency.
- Studies have shown that the majority of taxpayers would much rather have universal health care over the current system.
- By providing universal access, the severity of epidemics may be reduced or even eliminated as the number of disease carriers is reduced.
V. Conclusion
Health care, as mentioned earlier in the introduction, is ranked 2nd after the war in Iraq among issues Americans would like to hear their presidential candidates address. As in every other presidential campaign, health care reform has become one of the big issues of the 2008 campaign. Following the news, one might notice that different reform plans that have been proposed by candidates from both sides of the political divide. Mitt Romney, presidential candidate from the Republican Party says that the government is the source of the problem in health care today. According to Romney, the government should be removed from the picture entirely, and the people—the demographic not specified—should be free to choose what kind of health care plan they need. This is, by definition the free market health care system, which if one would reconsider is not much of a reform as it is an incremental change in the current system. Not much of universal health care is heard of, even among the Democratic presidential candidates. So far only Dennis Kucinich, has expressed the need for a full and drastic reform.
I personally find universal health care to be the most logical solution to this dysfunctional health care system. However, besides the invasion of Iraq, there has never been a drastic change in American public policy. I believe that this concept of incrementalism stems from the fear of a centralized government. For every voice that cries for governmental expansion for human welfare there is always a louder voice provoking fear of socialism. But should we really make unnecessary sacrifices, the welfare of an entire society, for an ideal that is classical liberalism?
In reality, if one understands how public policy is made in America than one should realize that the prospect of adopting a universal health care system is virtually impossible. Yes, universal health care is the most logical solution but as the current system is the system “the people” have chosen, a system in which incrementalism is like an inseparable limb, expecting that a drastic health care reform will happen is inevitably fruitless.
References
American College of Physicians (2004). The cost of lack of health insurance, 2004.Retrieved October 1, 2007, from http://www.acponline.org/hpp/cost.pdf
Andrews, M. (2007). The politics of healthcare. U.S. News & World Report, 143(11), 27.
British Broadcasting Corporation. (2005). Labour hails fall in MRSA cases, 2005.
Retrieved October 1, 2007, from http://news.bbc.co.uk/2/hi/health/4324281.stm
Center for Disease Control and Prevention (2007, June). Early releases of selected estimates based on data from the 2006 National Heath Interviews Survey. Retrieved October 1, 2007, from http://www.cdc.gov/nchs/earlyrelease/200706_11.pdf
The Commonwealth Fund. (2007). Employers provide health benefits to more than 160 million working Americans and family members, 2006. Retrieved October 1, 2007, from http://www.commonwealthfund.org/chartcartcharts/chartcartcharts_show.htm?do c_id=523155
Congressional Budget Office. (2007). Children’s health insurance program reauthorization act of 2007, 2007. Retrieved October 1, 2007, from http://www.cbo.gov/cedirect.cfm?bill=hr976&cong=110
Corning, P. (1969). History of mediare.
U.S. Social Security Administration, Office of Research and Statistics
Goodman, J. (2005). Five myths of socialized medicine. Cato Institute: Cato’s Letter Winter, 2005
Kant, P., & Rushefsky, M. (2006). Health care politics and policy in America.
Armonk, NY: M.E. Sharpe, Inc.
Lemons, J. S. (1969). The Sheppard-Towner Act: progressivism in the 1920s.
The Journal of American History, 55, no.4, 776-786
Lewin, M.E., & Baxter, R.J. (2007). America’s health care safety net: Revisiting the 2000 IOM report [Electronic version]. Health Affairs, 26(5), 1490- 1494
The Official U.S. Government site for people with Medicare (2007). Medicare Health Plans, 2007. Retrieved October 1, 2007, from http://www.medicare.gov/
Peters, B. G. (2007). American public policy: promise and performance.
Washington, DC: CQ Press
The Public Citizen. (2004). Study shows national health insurance could save $286 billion on health care paperwork, 2004. Retrieved October 1, 2007, from http://www.citizen.org/pressroom/release.cfm?ID=1623
Stoiber, S. A. (2006). National Health Insurance. From the Enclopedia of Public Health website. Retrieved October 1, 2007, from http://www.enotes.com/public-health-encyclopedia/national-health-insurance
U.S. Department of Health and Human Services. (2006). Information about persons covered by Medicare, Medicaid, or SCHIP, 2006. Retrieved October 1, 2007, From http://www.cms.hhs.gov/CapMarketUpdates/Downloads/2006CMSstat.pdf
Woolhandler, et al. (2003). Cost of health administration in the U.S. and Canada. New England Journal of Medicine 349(8).World Health Organization. (2000, June).
World Health Organization assesses the world’s health systems. Retrieved October 1, 2007, from http://www.who.int/inf-pr-2000/en/pr2000-44.html